 E-submission
E-submission
Search
- Page Path
- HOME > Search
Case Reports
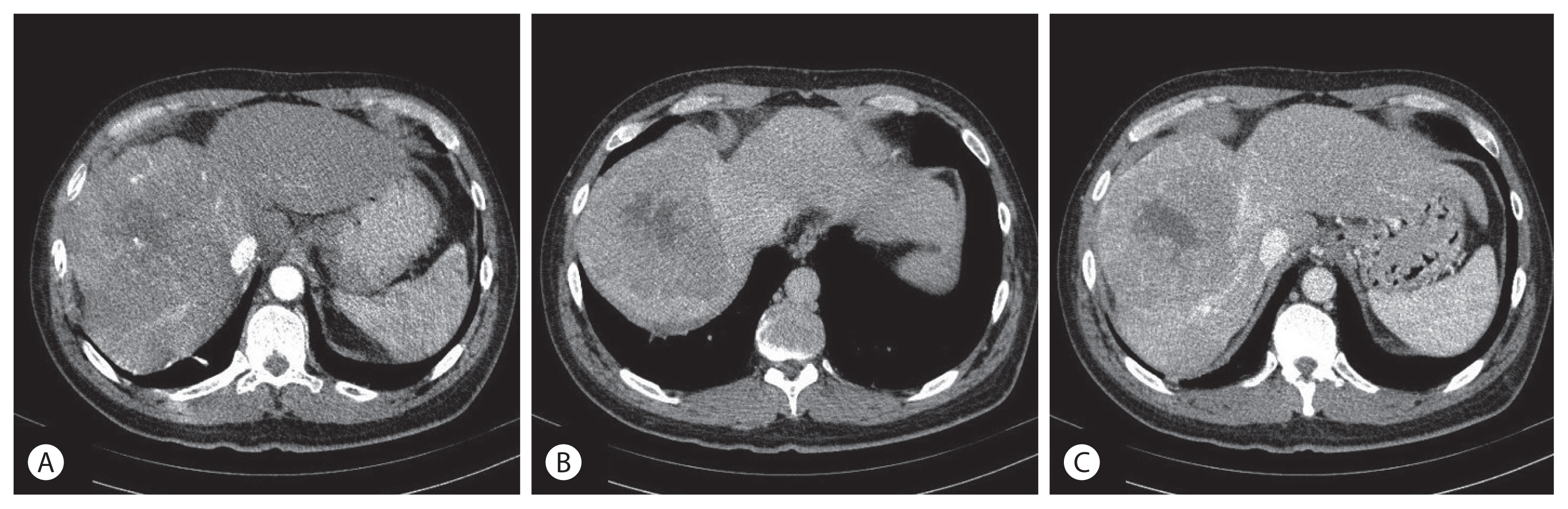
- Huge Hepatocellular Carcinoma Exhibiting a Complete Response after Stereotactic Body Radiation Therapy
- Kyung In Shin, Byoung Kuk Jang, Jin Hee Kim, Jae Seok Hwang
- J Liver Cancer. 2020;20(2):167-172. Published online September 30, 2020
- DOI: https://doi.org/10.17998/jlc.20.2.167
- 2,869 Views
- 99 Downloads
-
 Abstract
Abstract
 PDF
PDF - To date, there are limited data and little consensus on treatment strategies for huge hepatocellular carcinoma (HCC). Surgical resection provides significantly better survival than other modalities for single large HCC regardless of tumor stage. Recently, with technological advances in radiation therapy, stereotactic body radiation therapy (SBRT) is considered an alternative treatment option for HCC. Herein, we present a case of huge HCC that was successfully managed by SBRT. Transarterial embolization, previously performed in Russia, was incomplete. It was also not suitable for resection and transarterial chemoembolization. Although the rationale for radiotherapy in huge HCC was insufficient, SBRT was performed because no other treatment options were available. Additional radiofrequency ablation was performed for small HCC in a different segment, and radiological complete response (CR) was achieved. The CR was maintained over 4 years. Therefore, SBRT may be an alternative treatment option for large HCC that is not suitable for curative treatment.

- A Case of Hepatocellular Carcinoma with Portal Vein Tumor Thrombosis Treated by Hepatic Artery Injection Chemotherapy and Radiotherapy
- Sang Jin Kim, Byoung Kuk Jang, Jae Seok Hwang
- J Liver Cancer. 2017;17(2):158-162. Published online September 30, 2017
- DOI: https://doi.org/10.17998/jlc.17.2.158
- 2,644 Views
- 19 Downloads
- 1 Citation
-
Abstract
PDF
- External beam radiotherapy, transarterial chemoembolization and sorafenib are currently standard treatments for advanced hepatocellular carcinoma (HCC) with portal vein thrombosis. However, hepatic arterial infusion chemotherapy has been applied to advanced stage HCC with a view to improving the therapeutic effect. We experienced a case of advanced HCC with clinical complete response after hepatic artery infusion chemotherapy and radiation therapy and report that.
-
Citations
Citations to this article as recorded by
- A Case of Hepatocellular Carcinoma with Portal Vein Tumor Thrombosis Treated by Hepatic Arterial Infusion Chemotherapy and Radiotherapy
Jin Yong Lee, Jeong-Ju Yoo, Seong Joon Chun, Sun Hyun Bae, Jae Myeong Lee, Sang Gyune Kim, Young Seok Kim
Journal of Liver Cancer.2020; 20(1): 78. CrossRef
- A Case of Hepatocellular Carcinoma with Portal Vein Tumor Thrombosis Treated by Hepatic Arterial Infusion Chemotherapy and Radiotherapy
Review Article
- The Role of Combination of Transarterial Chemoebolization and Radiofrequency Ablation for Hepatocellular Carcinoma Treatment
- Byoung Kuk Jang
- J Liver Cancer. 2017;17(1):15-18. Published online March 31, 2017
- DOI: https://doi.org/10.17998/jlc.17.1.15
- 1,331 Views
- 24 Downloads
-
Abstract
PDF
- Recently, various combination therapies have been applied to the treatment of hepatocellular carcinoma (HCC). Among various treatment modalities, transarterial chemoembolization (TACE) and radiofrequency ablation (RFA) were combined to improve the therapeutic effect of RFA. The decrease of blood flow by TACE can increase the size of the ablation area by reducing heat loss during RFA. Based on these theoretical advantages, TACE and RFA combination therapy have been tried for the treatment of patients with HCC which is not feasible to be removed by surgery. However, TACE and RFA combination therapy has not been standardized by various protocols for each study. This review discusses the implications and role of this treatment, although there are several limitations to clearly demonstrate the indications and efficacy of TACE and RFA combination therapies.
Case Reports
- A Case of Early Multiply Recurred Hepatocellular Carcinoma after Surgical Resection in Patient Who Unprecedented Chronic Liver Disease
- Wang Yong Choi, Byoung Kuk Jang, Woo Jin Chung, Jae Seok Hwang
- J Liver Cancer. 2015;15(2):112-117. Published online September 30, 2015
- DOI: https://doi.org/10.17998/jlc.15.2.112
- 871 Views
- 4 Downloads
-
Abstract
PDF
- Hepatocellular carcinoma (HCC) have relatively well known causative factors such as chronic hepatitis B, chronic hepatitis C, alcoholic liver disease, Non-alcoholic fatty liver disease (NAFLD), liver cirrhosis and so on. Recently, interesting reports that HCC in the absence of cirrhosis or other chronic liver disease and HCC associated with NAFLD and metabolic syndrome are increasing in USA. So far, there is no report about these issues in Korea. We present a 65 yearold obesity male who had no preceding chronic liver disease history. He was diagnosed as primary HCC and the mass was removed completely. However, HCC recurred shortly after operation. Multiple recurred HCC were treated with transcatheter arterial chemoembolization. (J Liver Cancer 2015;15:112-117)
- A Case of Hepatocellular Carcinoma Presenting with Rib Metastasis
- Kyung In Lee, Young Lan Kwon, Yoon Jung Kim, Hye Jin Seo, Yong Jin Kim, Chang Wook Park, Eun Soo Kim, Byoung Kuk Jang, Woo Jin Chung, Kyung Sik Park, Kwang Bum Cho, Jae Seok Hwang, Jung Hyeok Kwon
- Journal of the Korean Liver Cancer Study Group. 2010;10(1):64-68. Published online June 30, 2010
- 580 Views
- 1 Download
-
Abstract
PDF
- Bone metastasis is not uncommon and shows poor survival in patients with hepatocellular carcinoma (HCC). We describe a case of HCC presenting with rib metastasis in a 54-year-old man. In spite of radiotherapy for rib metastasis, pain was sustained and size of lesions were increased. So we performd CT-guided percutaneous ethanol injection therapy (PEIT). Whenever new metastatic bone lesions were detected, we have done PEIT. However, abdominal CT scan at 25th month after diagnosis shows residual viable tumors in pelvic bone and multiple metastatic nodules in both lung. He is alive by taking conservative management for 27 months after diagnosis.
- A Case of Curative Resection of Advanced Hepatocellular Carcinoma After Localized Concurrent Chemo-Radiation Therapy
- Jee Suk Kwon, Jeong Eun Lee, Woo Young Park, Kyung In Lee, Eun Soo Kim, Byoung Kuk Jang, Woo Jin Chung, Kyung Sik Park, Kwang Bum Cho, Jaeseok Hwang
- Journal of the Korean Liver Cancer Study Group. 2009;9(1):67-70. Published online June 30, 2009
- 471 Views
- 1 Download
-
Abstract
PDF
- Advanced hepatocellular carcinoma (HCC) with portal vein thrombosis is not suitable candidates for surgical treatment at the most of diagnosis because of poor liver function, extensive tumor involvement of the liver, vascular involvement, and/or intra/extrahepatic metastasis. We attempted localized concurrent chemo-radiation therapy (CCRT) in patients having locally advanced HCC with left and main portal vein thrombosis. We report a case of locally advanced HCC patient who became surgically resectable by downstaging after localized CCRT. Localized CCRT was performed with a total radiation dose of 5,040 cGy (180 cGy×28 times) and hepatic arterial infusion of 5-fluorouracil (5-FU, 250 mg/day) and cisplatin (10 mg/day) for 5 days via implantable port system during the second and the fifth weeks of the radiotherapy. Marked contraction of HCC was noted on follow up computerized tomography (CT) after localized CCRT, and subsequently surgical resection with curative aim was performed. He was gave a additional transcatheter arterial chemoembolization (TACE) because follow up CT revealed intrahepatic metastasis at subcapsular portion of right hepatic lobe after 3 months of operation. The patient is in complete remission status without recurrence to date.
- A Case of Benign Hepatic Nodule Difficult to Differenciate from Hepatocellular Carcinoma
- Byoung Kuk Jang, Woo Jin Chung, Kyung Sik Park, Kwang Bum Cho, Jae Seok Hwang, Sung Hoon Ahn, Young Hwan Kim, Jung Hyeok Kwon, Yu Na Kang
- Journal of the Korean Liver Cancer Study Group. 2007;7(1):45-48. Published online June 30, 2007
- 559 Views
- 0 Download
-
Abstract
PDF
- Improved imaging techniques have led to increasing detection of hepatic nodules incidentally. In many cases, a lesion that has been detected by imaging studies is not sufficiently characteristic, or there are other clinical concern, so that an imaging guided percutaneous needle biopsy is performed for definitive diagnosis. But sometimes, there are diagnostic difficulty due to limited diagnostic samples. We report a case of diagnosis to benign nodule, but not confirmed specific disease, by repeated CT guided fine needle biopsy.
- Two Cases of Advanced Hepatocellular Carcinoma Showing Good Response to Hepatic Arterial Infusion Therapy
- Byoung Kuk Jang, Woo Jin Chung, Kyung Sik Park, Kwang Byum Jo, Jae Seok Hwang, Sung Hoon Ahn, Young Hwan Kim, Jin Soo Choi, Jung Hyuk Kwun
- Journal of the Korean Liver Cancer Study Group. 2006;6(1):60-64. Published online June 30, 2006
- 499 Views
- 0 Download
-
Abstract
PDF
- Prognosis of advanced hepatocellular carcinoma (HCC) treated by conventional therapies has been considered to be poor. Hepatic arterial infusion therapy (HAIT) has been tried for advanced hepatocellular carcinoma with portal vein tumor thrombosis or ineffective response to other treatment. We report two cases of advanced HCC showing good respense to transarterial chemoembolization and CT guided percutaneous ethanol injection therapy.
- Two Cases of Bone Metastasis of Hepatocellular Carcinoma without Intrahepatic Recurrence
- Byoung Kuk Jang, Woo Jin Chung, Kyung Sik Park, Kwang Bum Cho, Jae Seok Hwang, Sung Hoon Ahn, Young Hwan Kim, Jin Soo Choi, Jung Hyeok Kwon
- Journal of the Korean Liver Cancer Study Group. 2006;6(1):89-94. Published online June 30, 2006
- 488 Views
- 0 Download
-
Abstract
PDF
- Extrahepatic metastases of hepatocellular carcinoma (HCC) are now increasing due to prolonged survival. Extrahepatic metastases of HCC frequently develop in patients with more advanced stage and sometimes occur without intrahepatic recurrence. We report two cases bone metastasis of HCC without intrahepatic recurrence after treatment.
- A Case of Early Multiple Recurrences After Hepatectomy with Lymph Node Dissection in Hepatocellular Carcinoma with Lymph Node Metastasis
- Byoung Kuk Jang, Ki Min Kwun, Woo Jin Jung, Kyung Sik Park, Kwang Byum Jo, Jae Suk Hwang, Seong Hoon Ahn, Ku Jung Kang, Jung Hyuk Kwun
- Journal of the Korean Liver Cancer Study Group. 2004;4(1):62-66. Published online June 30, 2004
- 481 Views
- 1 Download
-
Abstract
PDF
- A 52-year-old man who underwent left hepatectomy with lymph node dissection due to hepatocellular carcinoma with lymph node metastasis. After 5 months of surgery, multiple recurrences were founded throughout the liver, lung, bones and intraperitoneal lymph nodes. The patient died of liver failure after rupture of recurrent hepatic tumor. From our experience, we reaffirmed that the prognosis of patients with nodal metastasis from hepatocellular carcinoma was generally poor, even after hepatic resection with lymph node dissection was performed.
 First
First Prev
Prev


 Follow JLC on Twitter
Follow JLC on Twitter